
Why the HHS Two-Part Test Is Now Influencing DEA Scheduling Decisions
By Jason Karimi
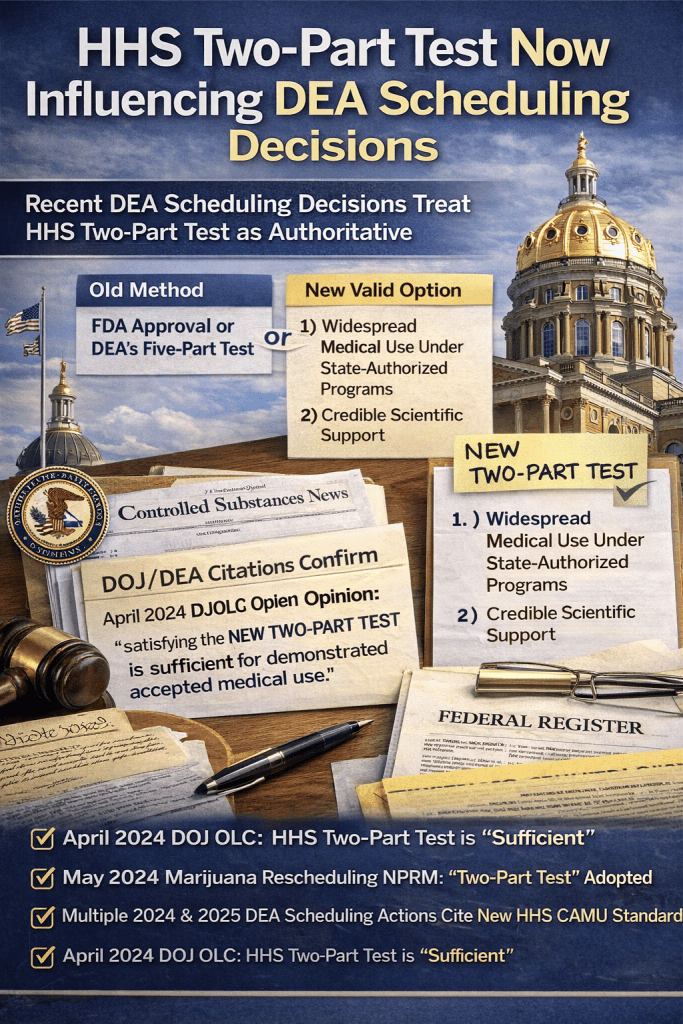
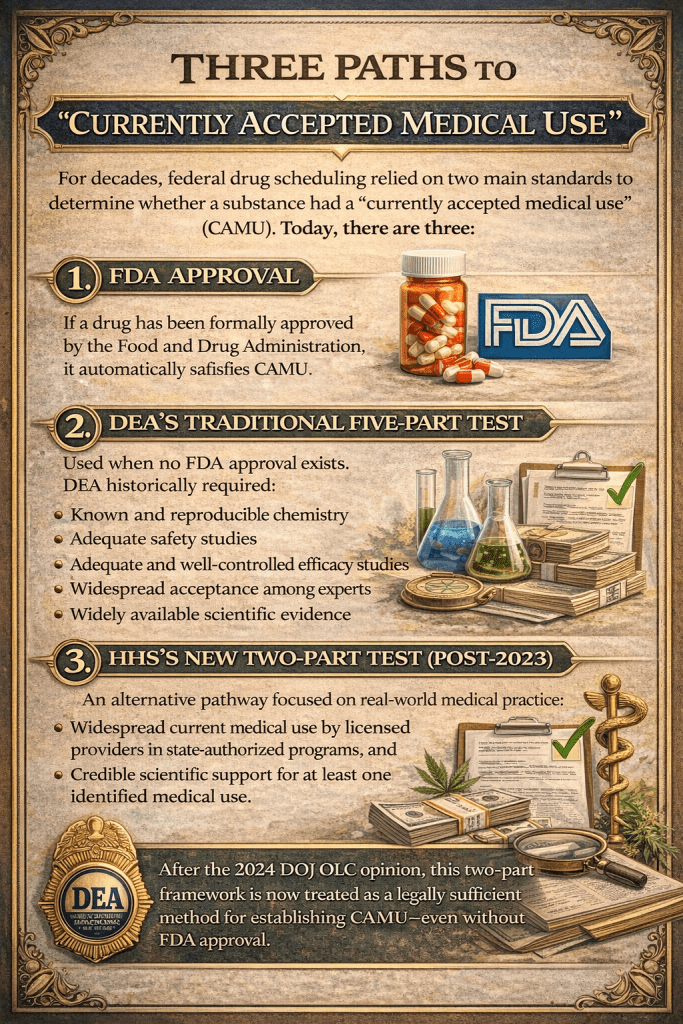
The Controlled Substances Act (CSA) has long required that a drug must have a “currently accepted medical use in treatment in the United States” before it can be placed outside of Schedule I. For decades, that determination was interpreted by the Drug Enforcement Administration (DEA), and relied on two main standards to determine whether a substance had a “currently accepted medical use” (CAMU). Today, there are now three standards:
1. FDA Approval
If a drug has been formally approved by the Food and Drug Administration, it automatically satisfies CAMU.
2. DEA’s Traditional Five-Part Test
Used when no FDA approval exists. DEA historically required the following five part test:
1. Known and reproducible chemistry
2. Adequate safety studies
3. Adequate and well-controlled efficacy studies
4. Widespread acceptance among experts
5. Widely available scientific evidence
This standard has proven difficult for many non-FDA-approved substances to meet.
But the legal landscape has shifted significantly in the past few years. A combination of new Department of Health and Human Services (HHS) criteria and a key Justice Department Office of Legal Counsel (OLC) opinion has given the DEA — and federal rulemaking — a new way to satisfy the “currently accepted medical use” test, even when FDA approval and the five-part test are not met.
3. HHS’s New Two-Part Test (Post-2023)
An alternative pathway focused on real-world medical practice:
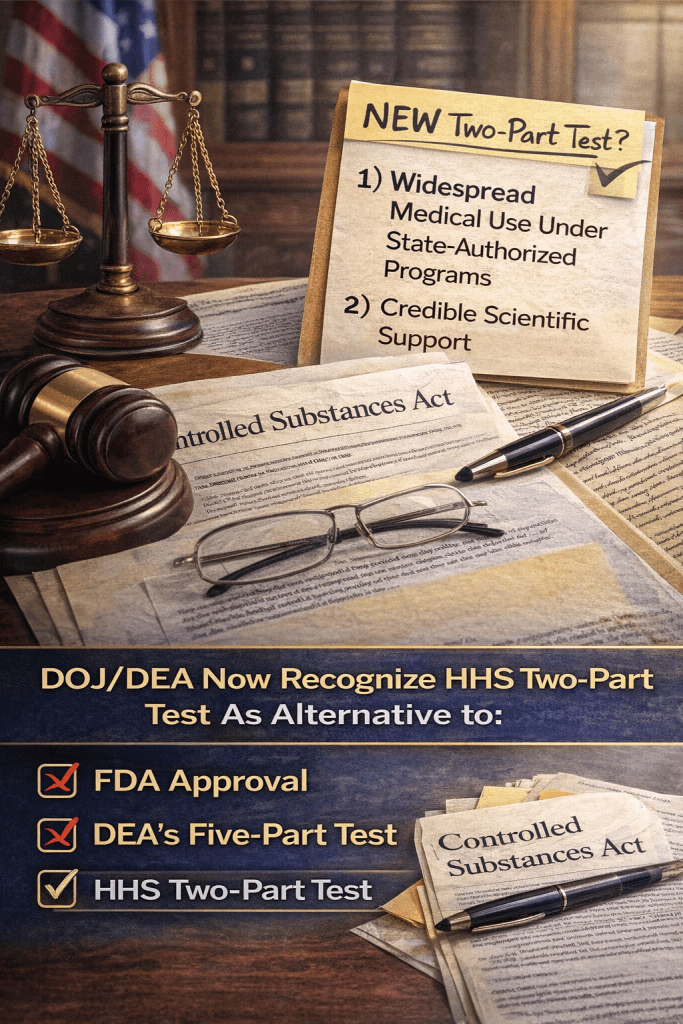
Widespread current medical use by licensed providers in state-authorized programs, and Credible scientific support for at least one identified medical use.
After the 2024 DOJ OLC opinion, this two-part framework is now treated as a legally sufficient method for establishing CAMU—even without FDA approval.
HHS’s Two-Part Test: A New Pathway
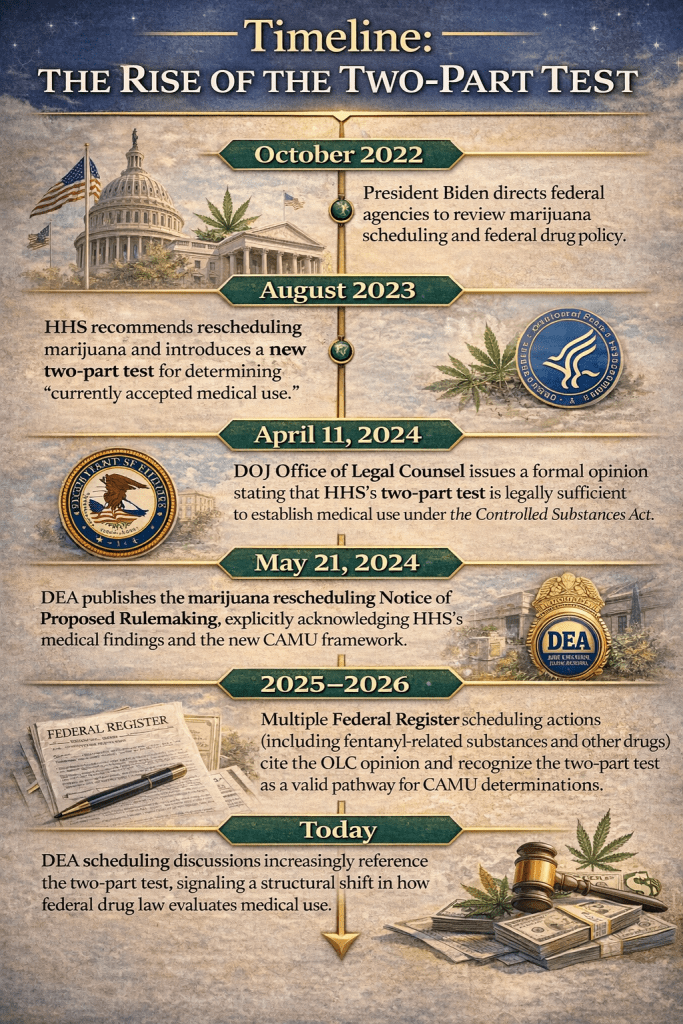
In August 2023, HHS formally recommended that marijuana be rescheduled from Schedule I to Schedule III and, in doing so, developed and applied a new two-part inquiry for determining whether a drug has a “currently accepted medical use” (CAMU) under the CSA.
Under that test:
1. There must be widespread current experience with medical use of the drug by licensed health care providers operating under implemented jurisdiction-authorized programs; and
2. There must be some credible scientific support for at least one of the medical uses identified under part 1.
This marked a clear departure from DEA’s rigid five-part test and reliance on FDA approval — a test that many critics long argued was too narrow and inconsistent with how certain drugs are actually used in medical practice.
OLC: The Two-Part Test Is Sufficient
The pivotal moment came in April 2024, when the Office of Legal Counsel (OLC) within the Department of Justice issued an opinion addressing whether satisfying HHS’s two-part test alone can establish that a drug has a currently accepted medical use under the CSA — even if it has not been approved by FDA and would not satisfy DEA’s five-part criteria.
In that opinion, OLC found that:
“Limiting the CAMU analysis to whether a drug has been approved by FDA or meets DEA’s five-part test is impermissibly narrow” and that satisfying HHS’s two-part inquiry is sufficient to establish that a drug has a currently accepted medical use under the CSA. Full quote:
“Limiting the CAMU analysis to whether a drug has been approved by FDA or meets DEA’s five-part test is impermissibly narrow. Satisfying HHS’s two-part inquiry is sufficient to establish that a drug has a currently accepted medical use under the CSA.”
— DOJ Office of Legal Counsel, 2024 OLC Marijuana Rescheduling Opinion
OLC’s opinion concluded that during a rulemaking process, HHS’s scientific and medical findings — including those based on the two-part test — are binding on DEA’s consideration and thereafter entitled to significant deference.
That was significant for two reasons:
1. It validated the HHS two-part test as legally adequate, even absent FDA approval.
2. It clarified that the CSA does not require strict reliance on DEA’s traditional five-part test.
This memorandum has since been cited by DEA in multiple Federal Register notices indicating how future scheduling actions may proceed.
How DEA Is Acknowledging the New Test
In the May 2024 Notice of Proposed Rulemaking (NPRM) to reschedule marijuana to Schedule III, DEA referenced the OLC opinion to explain the legal basis for considering HHS’s findings — including those derived from the two-part test — as part of the evidence that marijuana has a currently accepted medical use. Full quote:
“DEA accords binding weight to the scientific and medical determinations of HHS… including those reflected in the HHS Accepted Medical Use analysis.”
— Schedules of Controlled Substances: Rescheduling of Marijuana, 89 FR 30212, May 21, 2024
HHS’s two-part test would be sufficient to establish that a drug has a currently accepted medical use under the CSA.
For example, a December 2024 Federal Register notice examining certain fentanyl-related substances cited the OLC memorandum and stated that the two-part test, as articulated by HHS and endorsed by OLC, is a valid way to determine whether a drug has a currently accepted medical use:
“As the Department of Justice Office of Legal Counsel concluded regarding the HHS medical use evaluation, satisfying HHS’s two-part test would be sufficient to establish that a drug has a currently accepted medical use under the Controlled Substances Act.”
— Schedules of Controlled Substances: Placement of Seven Specific Fentanyl-Related Substances in Schedule I, 90 FR 12860, June 26, 2025
These citations show that the “two-part test” has moved from an academic proposal into the heart of federal regulatory discussions.
Another scheduling action in late 2025 similarly cites the OLC memo:
“HHS may apply its accepted medical use standard, which in the absence of FDA approval includes whether there is widespread medical use and scientific support. This standard, highlighted in the OLC memorandum, would be sufficient to demonstrate currently accepted medical use under the CSA.”
— Schedules of Controlled Substances Action, 90 FR 25910, Oct. 15, 2025
Again, this is not merely background, but part of DEA describing how modern “accepted medical use” evaluations can function:
When no FDA approval exists, DEA has traditionally applied a five-part test to determine whether a drug or substance has a currently accepted medical use… In a recent published letter in a different context, HHS applied an additional two-part test to determine currently accepted medical use for substances that do not satisfy the five-part test:
(1) whether there exists widespread, current experience with medical use of the substance by licensed health care providers operating in accordance with implemented jurisdiction-authorized programs, where medical use is recognized by entities that regulate the practice of medicine, and, if so,
(2) whether there exists some credible scientific support for at least one of the medical conditions for which part (1) is satisfied. On April 11, 2024, the Department of Justice’s Office of Legal Counsel… concluded that HHS’s two-part test would be sufficient to establish that a drug has a currently accepted medical use.
Source: https://public-inspection.federalregister.gov/2026-00954.pdf?
What these citations actually prove
Here’s what these excerpts show together:
✅ OLC formally backed the two-part test as sufficient to establish “currently accepted medical use” under the CSA.
✅ DEA is repeatedly citing OLC in Federal Register scheduling actions to explain how it evaluates medical use.
✅ DEA acknowledges that HHS’s findings based on the two-part test carry weight in scheduling evaluations.
✅ Federal Register rules are using language that equates the two-part test with an acceptable standard for accepted medical use — not just the old FDA/five-part approach.
What the rulemaking language does not yet say (but could)
No Federal Register scheduling decision so far has literally said:
“The two-part test itself is binding on DEA as a standalone legal requirement.”
However:
✔ HHS’s scientific/medical determinations have been treated as binding during the rulemaking process (OLC).
✔ DEA’s cited language shows that HHS’s standards are legitimate pathways DEA will consider.
This is essentially the legal battleground today:
Does “significant deference” equal full binding authority even after notice-and-comment? Courts have yet to definitively say.
What This Does — and Does Not — Mean
What It Does Mean:
– DOJ/DEA now have an explicitly recognized alternative pathway for establishing CAMU—even in the absence of FDA approval and without satisfying the five-part test.
– The HHS scientific and medical evaluation based on the two-part test plays a significant role in federal scheduling rulemaking.
What It Does Not Mean (Yet):
– It has not been universally declared that the two-part test itself is constitutionally binding on DEA in the same way (e.g., no court has ruled this outright, nor has DEA stated unwavering supremacy of that test alone).
– DEA still has ultimate authority to schedule, reschedule, or deschedule under the CSA — including on final rulemaking after notice and comment. Even with the influence of the two-part test and HHS’s findings, DEA retains final scheduling authority under the Controlled Substances Act.
However, the OLC opinion firmly places HHS’s scientific and medical determinations — including those derived from the two-part test — in a position of significant deference. Even after DEA initiates formal rulemaking, OLC states the agency “must continue to accord HHS’s scientific and medical determinations significant deference and may not undertake a de novo assessment” of them.
Implications for Future Scheduling Battles
This legal and regulatory evolution could reshape how a range of substances are evaluated under the CSA:
– Marijuana’s proposed rescheduling has thrust the two-part test into the mainstream, setting a precedent for how federal agencies approach “accepted medical use” determinations.
– Other non-FDA approved substances with widespread clinical use but limited formal trials (e.g., some psychedelics) may similarly benefit from this framework.
While courts and future administrative actions will ultimately refine these standards, the DOJ/DEA federal record now clearly acknowledges the two-part test as a viable (and in some cases sufficient) pathway for establishing medical use under federal drug law.
– Traditionally, DEA’s five-part test has been nearly impossible to satisfy for substances like cannabis because three of the five factors often couldn’t be met — a point courts have previously recognized.
– HHS’s two-part test was designed specifically to fill that gap where widespread clinical experience exists — even without large clinical trials or FDA approval.
This context clearly explains why the new test matters beyond just bureaucratic rearrangement.
Current limitations
No court has yet settled whether the two-part test must be binding post-NPRM.
DEA still retains ultimate statutory authority to decide scheduling under the Controlled Substances Act.
Footnote A (OLC memo):
Department of Justice, Office of Legal Counsel, Questions Related to the Potential Rescheduling of Marijuana (Apr. 11, 2024) (“…satisfying HHS’s two-part inquiry is sufficient to establish that a drug has a currently accepted medical use under the CSA.”).
Footnote B (Marijuana NPRM):
Schedules of Controlled Substances: Rescheduling of Marijuana, 89 Fed. Reg. 30212, 30215 (May 21, 2024) (“DEA accords binding weight to the scientific and medical determinations of HHS…”).
Footnote C (Fentanyl-Related Substances):
Schedules of Controlled Substances: Placement of Seven Specific Fentanyl-Related Substances in Schedule I, 90 Fed. Reg. 12860, 12863 (June 26, 2025) (“…satisfying HHS’s two-part test would be sufficient…”).
Footnote D (Oct. 2025 Notice):
Schedules of Controlled Substances Action, 90 Fed. Reg. 25910, 25913 (Oct. 15, 2025) (citing HHS’s accepted medical use standard and OLC memorandum).

Leave a comment