Cannabis and the Aging Brain: Science, Scheduling, and the Policy Consequences of New Data
By Jason Karimi | WeedPress | February 8, 2026

A new peer-reviewed study in the Journal of Studies on Alcohol and Drugs examined whether lifetime cannabis use is associated with differences in brain volume and cognitive function in middle-aged and older adults.
The media version of this story reads: cannabis may benefit aging brains.
The scientific version is more careful — and more interesting.
And the policy implications are unavoidable.
⸻
1️⃣ What the Study Measured
Researchers analyzed:
• Lifetime cannabis use history
• Neuroimaging data (regional brain volume)
• Cognitive performance measures
The focus population: middle-aged and older adults — not adolescents.
That distinction matters biologically and politically.
Adolescent neurodevelopment is uniquely sensitive. Midlife and aging brains operate under different neuroplastic and inflammatory conditions.
⸻
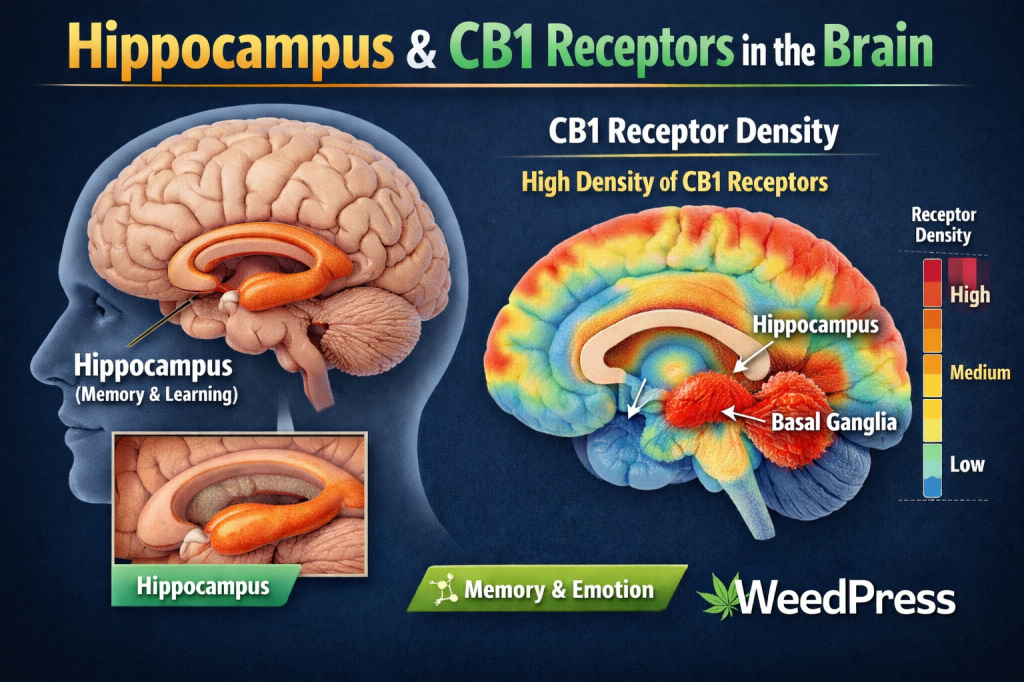
2️⃣ Brain Regions Identified
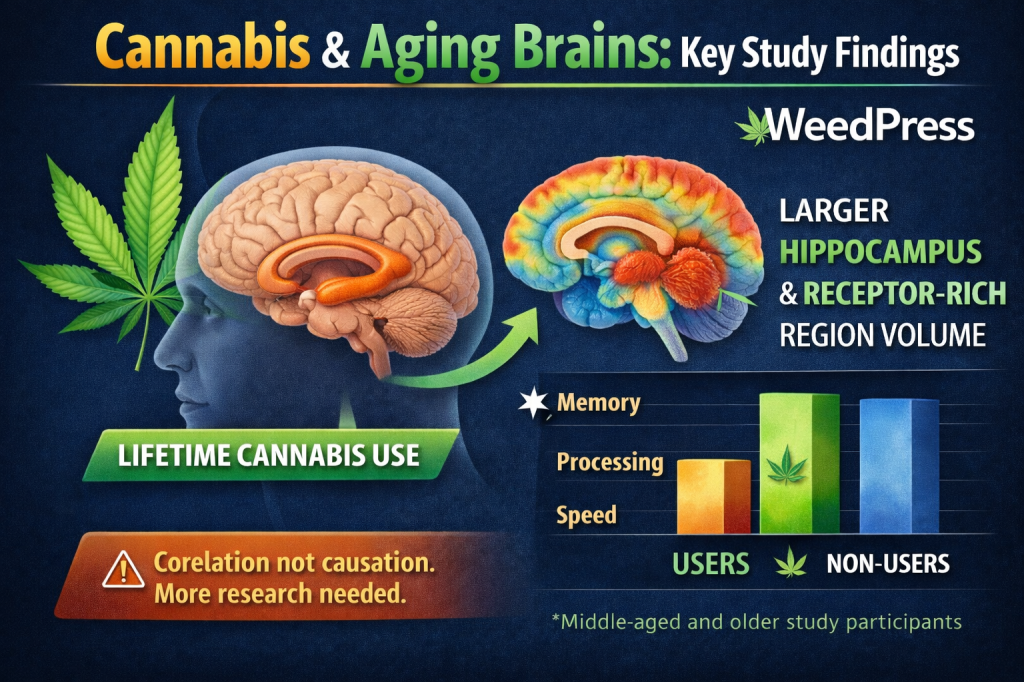
The study reports associations between lifetime cannabis use and larger volume in certain brain regions, including:
• Hippocampus (critical for memory consolidation)
• Basal ganglia components (motor and cognitive integration)
These areas are dense in CB1 receptors, the primary receptor through which THC exerts psychoactive and neuromodulatory effects.
“Larger volume” does not inherently mean “better.”
But in this dataset, regional volumetric differences were correlated with selected cognitive performance measures.
The key takeaway:
There was no uniform evidence of structural degeneration in older lifetime users.
⸻
3️⃣ Cognitive Findings
Participants with lifetime cannabis exposure did not show broad cognitive decline relative to non-users.
In some measured domains, associations trended toward preserved or better performance.
Important:
This is correlational, not causal.
But it contradicts prohibition-era messaging that cannabis use inevitably causes structural brain damage across the lifespan.
⸻
4️⃣ Biological Mechanisms (Hypothesized)
The endocannabinoid system regulates:
• Synaptic plasticity
• Neuroinflammation
• Stress response
• Excitotoxicity
CB1 receptors are heavily expressed in the hippocampus.
Preclinical research suggests cannabinoids may modulate:
• Inflammatory signaling
• Oxidative stress
• Neural excitability
Whether these mechanisms translate into long-term structural preservation in humans remains unresolved.
This study does not prove neuroprotection.
It suggests the relationship is more complex than harm-only narratives.
⸻
Policy Forward: Why This Matters for Federal Scheduling
Cannabis remains federally classified as Schedule I under the Controlled Substances Act — defined as:
High potential for abuse
No accepted medical use
Lack of accepted safety under medical supervision
Scientific literature increasingly complicates those assertions.
1️⃣ The “No Accepted Medical Use” Standard
Federal rescheduling analysis under HHS and DEA review considers:
• Scientific evidence of pharmacological effect
• Risk profiles
• Accepted medical use criteria
Data showing:
• Absence of structural neurodegeneration in aging populations
• Potential preservation of brain volume in receptor-dense areas
• No broad cognitive impairment in older adults
Undermines simplistic safety arguments used to justify Schedule I status.
Rescheduling discussions are not solely about youth risk. They consider adult safety data.
This study contributes to that record.
⸻
2️⃣ Abuse Liability vs Neurotoxicity
Schedule I implies high abuse potential and severe risk.
Neurotoxicity evidence matters.
If longitudinal data continue to show:
• No accelerated neurodegeneration
• No consistent cognitive decline in adult cohorts
It weakens claims that cannabis poses inherent long-term neurologic harm equivalent to Schedule I positioning.
Comparative frameworks matter here:
Alcohol — Schedule None
Opioids — Schedule II
Cannabis — Schedule I
Scientific consistency becomes harder to defend as more data accumulate.
⸻
3️⃣ Federalism Stress Test
States have legalized cannabis across medical and recreational frameworks.
Federal classification remains static.
When peer-reviewed data suggest:
• Adult use is not broadly neurodegenerative
• Aging populations are not demonstrating collapse in function
The federal-state misalignment grows more conspicuous.
Rescheduling debates increasingly hinge on empirical harm data.
Studies like this become administrative record inputs.
⸻
4️⃣ The Caution
This study does not justify:
• Marketing cannabis as neuroprotective
• Claiming cognitive enhancement
• Public health minimization
Rescheduling analysis weighs:
• Dose
• Mode of administration
• Population vulnerability
• Public safety metrics
But the absence of widespread structural harm in aging cohorts is relevant to that calculus.
⸻
Scientific Bottom Line
The data suggest:
• Lifetime cannabis use in middle-aged and older adults is not uniformly associated with brain atrophy.
• Certain regions rich in CB1 receptors show larger volume in this dataset.
• Cognitive performance did not show broad impairment.
This complicates prohibition-era neurodegeneration claims.
It does not close the case.
It reframes it.
⸻
Policy Bottom Line
As federal agencies review cannabis classification:
• Structural brain data matter.
• Lifespan differentiation matters.
• Adult safety evidence matters.
Science does not automatically dictate policy.
But weak harm narratives cannot indefinitely sustain Schedule I architecture in the face of accumulating peer-reviewed nuance.
The aging brain is now part of the rescheduling record.
⸻
WeedPress
Statute. Structure. Systems.

📖 2 Timothy 2:15 (KJV)
“Study to shew thyself approved unto God, a workman that needeth not to be ashamed, rightly dividing the word of truth.”
Proverbs 23 (KJV)
16 A fool’s wrath is presently known: but a prudent man covereth shame.
17 He that speaketh truth sheweth forth righteousness: but a false witness deceit.
18 There is that speaketh like the piercings of a sword: but the tongue of the wise is health.

Leave a comment