For more than seventeen years, the central argument advanced on WeedPress has been straightforward: medical cannabis cannot achieve real legitimacy or stability while operating in a permanent state of federal prohibition. State programs alone, no matter how well-intentioned, were always structurally limited by the Controlled Substances Act’s Schedule I classification and the absence of workable exemption pathways. The solution was never simply more state laws. It was the development and activation of federal exemption architecture.
That argument is now being tested in real time.
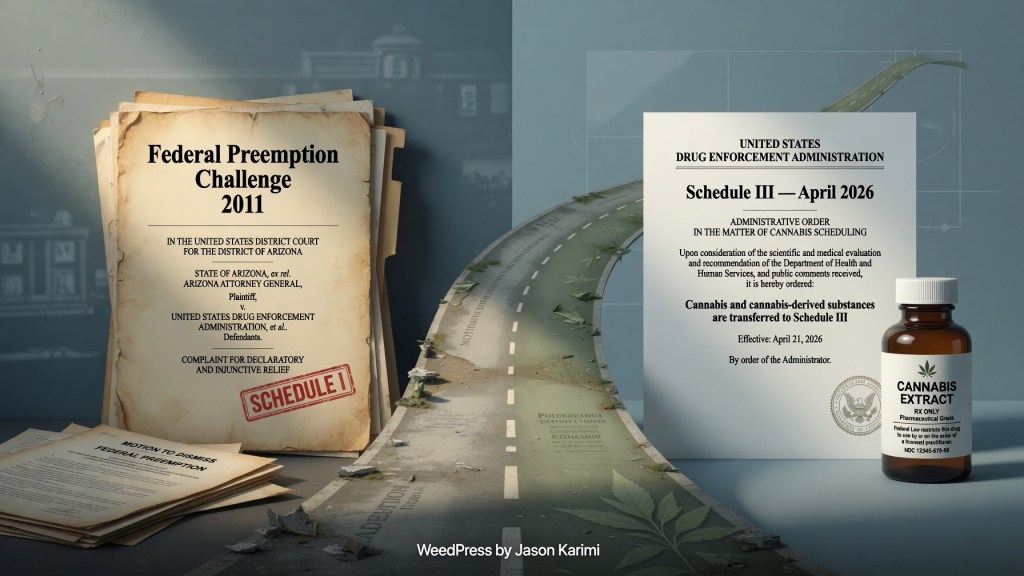
In 2011, when Arizona’s medical cannabis law faced a direct legal challenge from the state’s governor, the core dispute turned on federal preemption and the lack of any meaningful federal exemption mechanism.¹ Similar tensions were already visible in other states. At the time, most advocacy focused on passing state medical programs and hoping federal enforcement would remain lax. The harder structural questions — how state medical cannabis could ever coexist with the federal Controlled Substances Act without constant legal vulnerability — received far less attention.
WeedPress documented these early conflicts and consistently argued that sustainable medical access required explicit federal recognition through exemption authority, particularly under provisions such as 21 U.S.C. § 822(d).² Early legal and policy work, including challenges to state-level barriers and direct engagement with federal exemption arguments, emphasized that Schedule I status was not merely symbolic. It was the primary obstacle preventing medical cannabis from functioning like other recognized medicines in institutional settings, financial systems, and federal programs.³
In April 2026, the federal government took a significant step in that direction. The Drug Enforcement Administration issued a final order moving certain FDA-approved marijuana products and marijuana subject to qualifying state medical cannabis programs from Schedule I to Schedule III.⁴ This action represented the first formal federal acknowledgment that marijuana, when regulated under state medical programs, possesses accepted medical use and lower abuse potential than Schedule I criteria allow.
For those who spent years making the case that federal exemption pathways were both legally available and practically necessary, this development constitutes partial validation. The long-standing claim that medical cannabis could not remain permanently trapped in Schedule I while states operated medical programs has been vindicated in part. The federal government has now recognized, through regulatory action, what state medical cannabis laws had already asserted for years.
Yet the validation remains incomplete.
Schedule I still governs most cannabis, including personal cultivation, non-FDA-approved products, and use outside narrow state-licensed medical channels. The April 2026 order created a limited pathway for certain state-regulated medical products while leaving broader questions unresolved. Nursing homes and other healthcare facilities continue to face conflicting signals. South Dakota law, for example, contains strong language treating qualifying patient use as equivalent to other medications, yet simultaneously permits healthcare facilities to prohibit or severely restrict medical cannabis on their premises.⁵ This structural tension was originally justified by the realities of full federal prohibition. That justification has now been substantially weakened.
The human stakes of these lingering gaps are visible in cases such as the Iowa nursing home proceeding involving a 91-year-old resident threatened with eviction for using medical cannabis in accordance with state law.⁶ Similar conflicts have arisen in multiple states where facilities cite outdated federal concerns to deny access to patients who have no realistic alternative living arrangements. These situations are not peripheral. They are the direct result of medical cannabis laws written during an era when federal Schedule I status made accommodation legally risky for institutions receiving federal funding.
The April 2026 federal action has not eliminated these problems, but it has changed the analysis. What was once a difficult federal-state conflict has narrowed into a question of state policy choice. South Dakota, like other states, now has the opportunity — and arguably the obligation — to review its Medical Cannabis Act and implementing regulations in light of the new federal classification. Provisions that were written to manage the risks of full prohibition may no longer be necessary or defensible.
The work that began with early analysis of preemption fights and exemption architecture has reached a new stage. The federal government has taken a meaningful step toward recognizing medical cannabis. The remaining task is to complete the transition: removing Schedule I for medical use where it no longer fits, activating available exemption authorities more broadly, and updating state laws so that the patients the programs were created to serve are not left behind in institutional settings.
Seventeen years of consistent focus on federal exemption architecture has brought the movement to this point. The next phase will determine whether that architecture is fully built or left half-finished.
Footnotes
¹ WeedPress, “Arizona Governor Sues to Block Medical Cannabis Law Citing Federal Preemption Concerns” (2011) (analyzing Governor Brewer’s legal challenge to Arizona’s medical cannabis program and the preemption arguments centered on the absence of federal exemption mechanisms). https://weedpress.org/2011/08/03/arizonas-medical-marijuana-lawsuit-has-no-merit/
² WeedPress articles and policy analysis from 2011 documenting early state-federal conflicts and the need for workable CSA exemption pathways under provisions such as 21 U.S.C. § 822(d).
³ Early legal and advocacy work, including challenges and public commentary around 2011, emphasizing that Schedule I status created structural barriers for medical cannabis programs beyond simple enforcement discretion.
⁴ Schedules of Controlled Substances: Rescheduling of Food and Drug Administration Approved Products Containing Marijuana From Schedule I to Schedule III; Corresponding Change to Permit Requirements, 91 Fed. Reg. 22714 (Apr. 28, 2026) (2026-08176).
⁵ SDCL 34-20G-22 (pharmaceutical equivalence language); SDCL 34-20G-25.1 (authorizing healthcare facilities to restrict or prohibit medical cannabis on facility grounds).
⁶ Iowa Capital Dispatch, “Nursing Home Takes Regulators to Court Over Resident’s Eviction” (June 4, 2026), https://iowacapitaldispatch.com/2026/06/04/nursing-home-takes-regulators-to-court-over-residents-eviction/ (detailing proceedings involving a 91-year-old medical cannabis patient facing eviction from a nursing home).
⁷ See generally SDCL ch. 34-20G (Medical Cannabis Act) (original structure reflecting federal prohibition-era constraints on institutional settings).
⁸ 91 Fed. Reg. 22714, supra note 4.
⁹ Id. (limiting Schedule III treatment to FDA-approved products and marijuana subject to qualifying state-issued medical marijuana licenses).
¹⁰ SDCL 34-20G-25.1 (facility discretion to prohibit consumption on grounds).
¹¹ See reporting on the Iowa nursing home eviction case and related proceedings involving a 91-year-old medical cannabis patient (2024–2026).
¹² SDCL 34-20G-22.
¹³ 91 Fed. Reg. 22714, supra note 4.
¹⁴ See analysis of post-rescheduling implications for healthcare facilities and long-term care settings (2026).
¹⁵ Iowa Capital Dispatch, supra note 6.
¹⁶ SDCL 34-20G-25.1.
¹⁷ See broader pattern of institutional resistance to medical cannabis access in states with medical programs, including cases where federal funding concerns were cited even as federal classification evolved.
¹⁸ 91 Fed. Reg. 22714, supra note 4.
¹⁹ SDCL ch. 34-20G (structural provisions reflecting prohibition-era compromises).
²⁰ See evolving legal and policy discussion regarding the need for states to update medical cannabis frameworks following federal rescheduling developments.

Leave a comment